


Key takeaways
- Patients are increasingly leaving emergency rooms without being seen. This causes knock-on effects impacting patients, providers, and health systems.
- More than one-third of ERs have faced temporary closures or reduced hours since 2019. This harms patient wellbeing and leads to crowed ERs and overburdened providers elsewhere.
- Rerouting patients to more appropriate care works for patients, providers, and decision-makers. Unlocking capacity in emergency rooms drives long-term network benefits.
To solve Canada’s emergency department (ED) challenges, we first need to understand them.
Patients, providers, and networks each navigate unique barriers to emergency care. Despite Canada’s public health expenditures ranking among the world’s highest, the country’s primary care access ranks below most global peers. This leads many patients to seek emergency care when clinics or pharmacies would more effectively address their issues. The results is overcrowded emergency rooms, long wait times, and overburdened staff.
The solution: reroute patients from EDs to more appropriate care settings in real-time.
Explore three key illustrations describing the situation below, and one more showcasing how we will solve the problem.
Patients are leaving emergency rooms without being seen
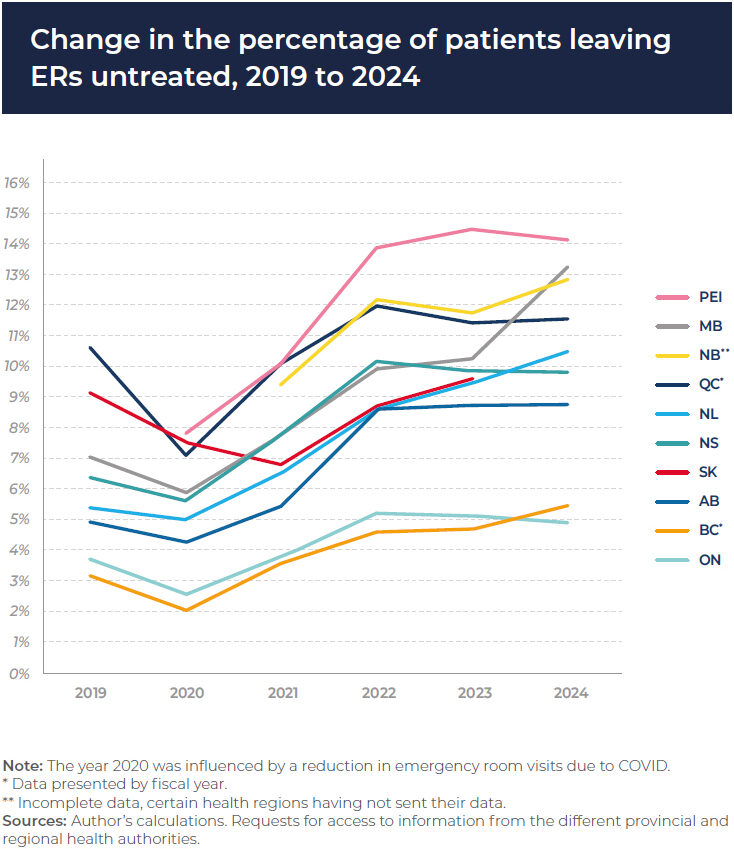
Across Canada, patients are increasingly walking into EDs and leaving before receiving care. This data from IEDM shows the percentage of patients leaving without being seen increased in most provinces from 2019–24. Prince Edward Island, New Brunswick, and Manitoba saw double-digit exit rates with PEI peaking at roughly 1 in 7 patients giving up on their ED care.
- Why patients leave: Long wait times—5.5 hours per visit nationally between 2024–25—lead patients to exit EDs to wait, self-treat, or seek alternative care options.
While COVID-19 temporarily suppressed ED visits in 2020, the trend quickly reversed. Wait times increased, ED volumes rebounded, and overcrowding returned. In Ontario, the Auditor General reported that some hospitals saw up to 14% of patients exit without care in 2023. Long wait times were cited as the main reason.
Why this matters: Patients who leave EDs may see their issues worsen. This risks their wellness, leading to further health problems and greater system strain.
The Quebec government redirects 800+ patients daily to more appropriate care.
Unplanned closures and long-lasting reductions in hours
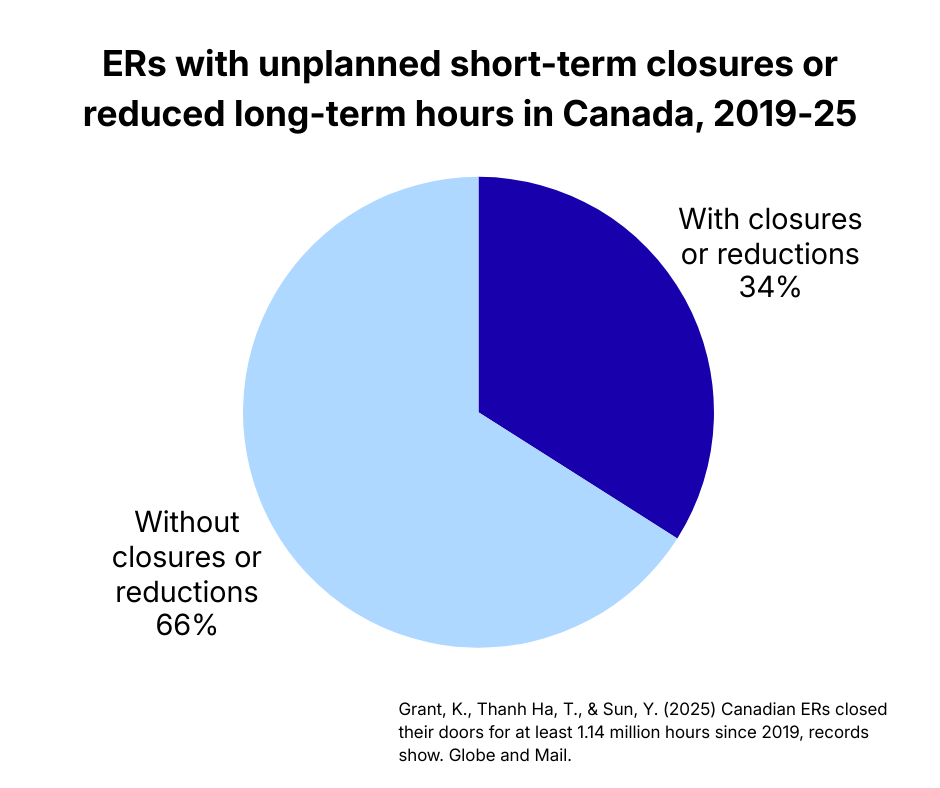
According to the Globe and Mail, at least 34 per cent of Canadian ERs had an unplanned, short-term closure or a planned, long-lasting reduction in hours since from 2019–25.
These closures and reductions span urban and rural communities nationwide. ED patients are forced to travel further to find care, which increases wait times elsewhere. The risk of delays in critical care increases too. The “domino effect” of ED closures and reductions leads to declining care outcomes for patients today and tomorrow. These closures erode public trust in local healthcare infrastructure and health governance.
Here are three key causes of ED disruption:
- Staffing shortages force operations to cease or limit their capacity.
- Burnt-out providers managing more patients with fewer support staff can’t fill the care gap alone.
- Overreliance on locum or temporary providers that create unmanageable barriers to care when care teams become understaffed.
Why this matters: For policy decision-makers, the 34% closure rate reflects system issues that threaten the wellbeing of all patients. Canadians will be stuck managing declining care consequences without innovative change.
More overtime hours lead to higher burnout
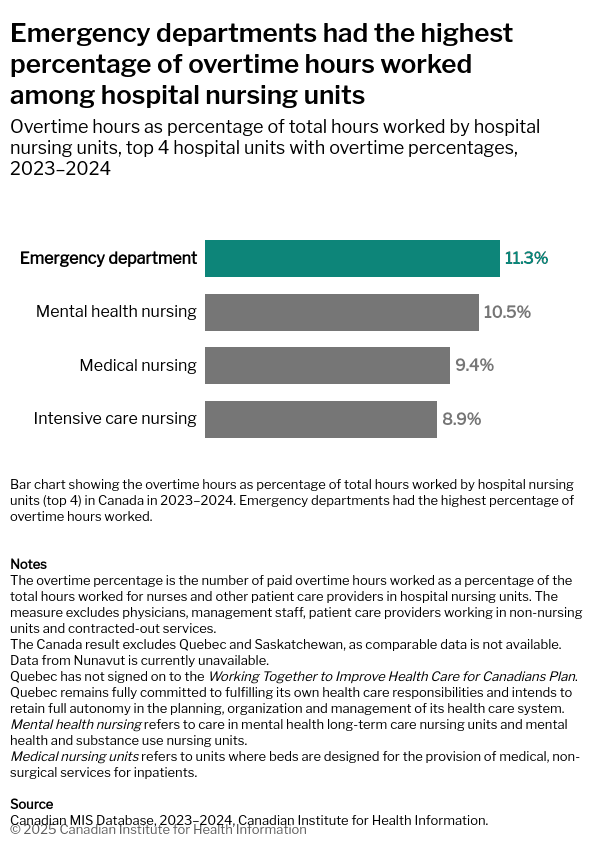
These findings from CIHI highlight increased strain on ED nurses compared to other nursing departments.
Healthcare professionals in EDs are especially susceptible to burnout due to the intense demands of their roles. Overtime creates higher pressures on nurses and physicians to perform. Many Canadians go to EDs because they don’t have access to a regular doctor; today, 5.9 million adults in Canada are without reliable access to primary care. This leads ED staff with more patients to support without requisite increases in fellow care staff.
This structure is unsustainable. Rising attrition rates due to overwork cause a negative feedback loop where staff become burnt-out, so they decide to leave the profession, which leads to increased work for existing staff. Patients lose when their care providers struggle to be well.
Why this matters: High overtime drives burnout, inflates labor costs, and reduces care quality. This impacts Canadians throughout the care continuum.
CHUM reduced time spent scheduling by 98% using Petal.
Solution: Rerouting patients to more appropriate care settings
Unlocking capacity in emergency rooms drives long-term network benefits.
Petal Patient Hub reroutes ED patients to more appropriate care settings like clinics and pharmacies in real-time. Patients, providers, and decision-makers achieve better outcomes when their needs are met efficiently.
Here are key findings from an independent study into Patient Hub’s impact:
- $2.3M per week in system-wide economic value
- 814,000+ ED visits avoided and 353,000+ redirected to primary care
- 12.5% fewer low-acuity ED visits (CTAS 4–5) compared to pre-Hub levels
When your health network is innovative, you meet today’s challenges and stabilize tomorrow’s growth.
Reduce ED overcrowding for patients and staff:


