


Key takeaways
- Inefficiencies are often hidden. Administrative workload, such as staff scheduling and cross-team communication, pulls physicians away from patient care and contributes to frustration and fatigue.
- Perceived unfairness in scheduling accelerates burnout. Even small imbalances in shift distribution, especially around nights and weekends, erode trust. Morale declines without clear rules and transparency as inequities become entrenched.
- Lack of visibility across systems and data prevents better decisions. Disconnected systems and underused data leave schedules unoptimized and risks unidentified. Inefficiencies persist as organizations are forced into reactive rather than proactive management.
In an era where time must be maximized to stretch healthcare budgets, wasting time on schedules is unsustainable.
Most physicians and administrators work hard to build effective schedules. Yet, 75% of physicians in Canada say their administration workload limits patient care. Manual scheduling is a key driver of this burden.
Manual scheduling pulls valuable time away from already busy physicians. This often becomes a source of fatigue, stress, and frustration among healthcare leaders responsible for patient wellbeing.
Burnout naturally follows. In Canada, 90% of nurses report some level of burnout and 60% of Quebec physicians show signs of burnout while 53% of physicians say admin workload has increased in the past 12 months. Addressing scheduling challenges will ease the burden facing these providers.
Read on for five scheduling mistakes that burnout physicians to start transforming your scheduling efficiency.
1) Relying on manual scheduling systems
Manual scheduling through Excel spreadsheets, email chains, text messages, and pager outreach introduces a level of friction that compounds over time.
Picture this: A schedule changes at 9:00 PM. An administrator updates a spreadsheet, emails three physicians, and sends two follow-up texts. One reply comes the next morning. Another never comes.
The gap remains.
By the time coverage is confirmed, hours have been spent coordinating what should have taken minutes.
Every schedule change triggers a cascade of updates. A single shift swap requires multiple follow-ups and revisions across a myriad of documents. What should be a simple adjustment becomes a time-consuming coordination effort.
- Did you know that nearly 90% of doctors in Ontario say they must use faxes to share patient information with other providers? Technological solutions are worth investment for forward-looking teams.
Phone call-outs are another hidden drain. When a gap appears in the schedule, administrators often spend hours calling physicians to find coverage. This is a 20th century solution to 21st century problems. Every minute spent working down call lists is time better spent supporting on-site teams and patients.
Of course, this burden shifts onto physicians. Doctors are often pulled into the coordination process, responding to messages, negotiating swaps, or tracking changes. Instead of focusing fully on patient care or recovery between shifts, they manage logistics. Over time, this creates a low-grade but persistent form of burnout. Physicians feel like they’re always “on,” even outside clinical hours.
Manual systems may seem cost-effective on the surface, but they quietly erode efficiency and well-being. The time spent managing schedules and the frustration they create add up quickly. In a system already under pressure, these inefficiencies are no longer sustainable.
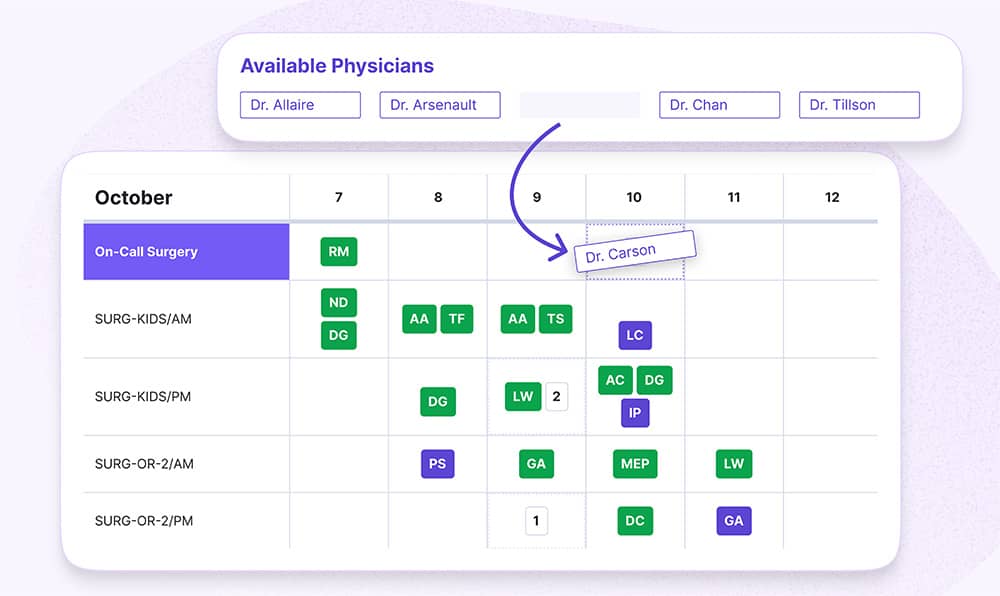
Solution: Empower physicians to claim and swap shifts by centralizing visibility for access on-site or remote. Automate shift management to accelerate the shift distribution process. Everyone sees available shifts, and everyone sees who takes them.
2) Creating inequitable schedules (even unintentionally)
Fair shift distribution precedes effective care.
It spans physician satisfaction, reducing burnout, and consistent patient care. Staffing shortages and rising patient volumes are common, and workforce management strategies that prioritize equity are essential.
Without a clear process, inequities creep in. Physicians and administrators become fatigued, and retention issues build, leading to fewer physicians and worsening care.
For example, perhaps certain physicians are always assigned weekend shifts because they always do these, or others are given lighter rotations due to historical preferences that were never revisited. Over time, these patterns solidify into imbalance.
Equally important is the consideration of individual physician preferences. Some physicians may prefer early shifts, fewer weekends, or specific types of assignments due to personal responsibilities or professional goals. When these preferences are not systematically captured and respected, dissatisfaction grows.
Physician leaders should ask:
- How are high-burden shifts weighted?
- How should nights and weekends be distributed?
- How do specialty constraints influence eligibility?
- How are new hires onboarded into rotations?
There’s no way to assess the success or impact of your scheduling efforts without defining targets or expectations. The result is that some physicians consistently receive undesirable shifts or heavier workloads.
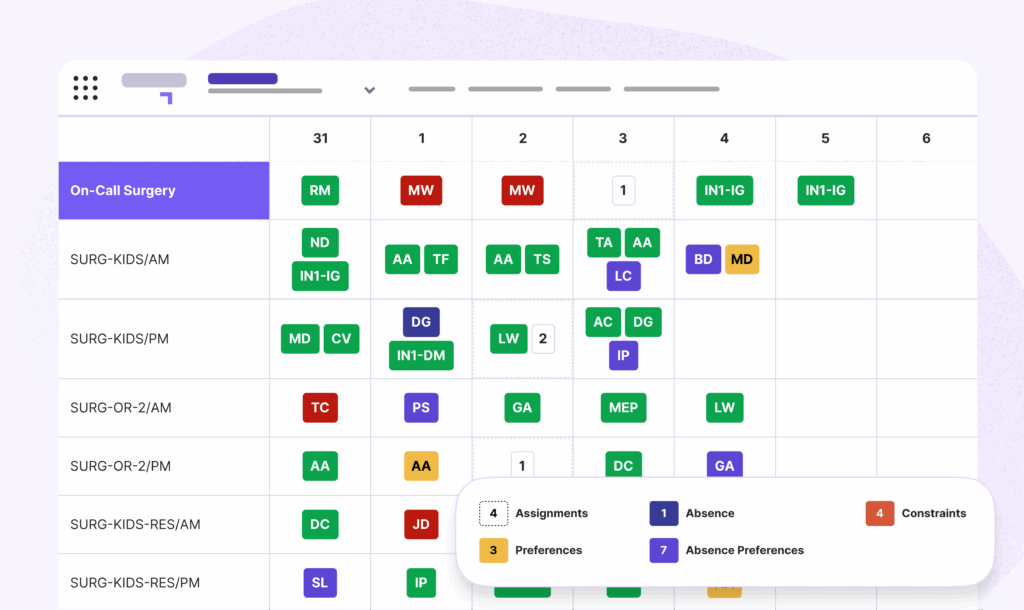
Solution: Perceived fairness drives morale. Track shift distribution across nights, weekends, holidays, and high‑demand duties. Build preferences into the system to ensure providers know their needs are recognized, and the system considers these needs.
37,000+ physicians leverage Petal Workforce to reduce scheduling burden.
3) Overloading your most reliable physicians
Every healthcare organization has its most dependable physicians. But relying on these top performers for the long term will burn them out and disrupt the team’s effectiveness.
This dynamic creates a negative feedback loop. As these physicians become overworked, their availability and energy decrease. Fatigue impacts performance, which in turn affects patient care, worsening patient outcomes, and creating further health issues that the system needs to solve.
Let’s frame the cultural effect on teams:
- Reliability leads to more work rather than recognition or balance;
- Physicians may begin to disengage strategically by doing less to avoid burden;
- And then trust erodes across the group.
Still, it’s understandable why administrators and top performers drive the status quo. It appears to be the best way to overcome pressure, including burden through unsustainable scheduling, and it allows patients to be cared for during the short term.
Patients feel the impact. When key physicians are stretched thin, wait times increase, and continuity of care suffers. The system becomes less resilient. Burnout becoming concentrated among the strongest contributors will not promote system success.
Solution: Introduce a rotating “coverage responsibility” model where all physicians take turns being the first point of contact for open shifts or last-minute gaps. This spreads the burden more evenly and normalizes participation. Top performers don’t feel like they need to be shift heroes.
CHUM reduced scheduling time by 98%.
4) Scheduling in digital silos
In 2025, 85% of Canada healthcare professionals reported losing time due to incomplete or inaccessible patient data.
Rather than allowing information to flow—securely—Canada’s health data lives in digital silos. This means a high volume and variety of patient data is stored in disconnected locations and systems. In turn, providers, patients, researchers, insurers, and health authorities all struggle to make effective, informed decisions.
Inevitably, patients pay the highest price of self-contained IT systems. Their ability to receive care is slowed when providers are slowed. Physicians absorb system inefficiencies, and then patients feel the impact through longer wait times and worsening care outcomes.
- Did you know that 8 in 10 Canadians want to view their health information electronically, but only 3 in 10 say they can?
These silos often create bottlenecks in one area while leaving unused capacity in another. For example, a physician may be overloaded with hospital shifts while having under-utilized availability during clinic time.
Additionally, this fragmentation complicates communication. Updates in one system may not reflect in another, leading to inconsistencies and confusion. This confusion drains time and energy from clinicians. They’re constantly forced to context-switch between different roles and schedules with little coordination.
Without stronger collaboration across systems and provinces, coordination breaks down at the operational level.
Solution: Healthcare IT systems must “talk” to each other to break down digital silos. When information flows securely, physicians’ lives are simplified and patient wellbeing improves. Integrate data-driven healthcare solutions to create an interconnected ecosystem and enable real-time monitoring.
5) Underutilizing workforce data
Healthcare organizations generate vast amounts of scheduling and workforce data—but too often, that data goes unused.
Without visibility into key metrics, it’s difficult to understand who is overworked and who may be underutilized. Schedules are created and adjusted based on immediate needs rather than informed insights. As a result, imbalances persist unnoticed.
Data is a critical resource for learning about operations. It reveals:
- Patterns in overtime.
- Weekend distribution.
- Workload intensity.
- Overall burden.
These insights are essential for identifying risks before they escalate into burnout.
A physician consistently taking extra shifts may not raise concerns until they reach a breaking point. Similarly, uneven distribution of undesirable shifts may go missed if not tracked systematically.
This lack of visibility also limits accountability. Without clear data, fairness is nearly impossible to achieve. Decisions may rely on anecdotal feedback rather than objective evidence. Over time, this creates a reactive environment. Issues are addressed only after they become urgent, rather than being prevented through proactivity.
In contrast, organizations that leverage workforce data make more informed, balanced decisions. They identify trends. They adjust schedules proactively. Workloads are distributed more equitably. When physicians understand how schedules are created and see that decisions are grounded in objective information, trust increases.
Solution: On a quarterly basis (at least), review key indicators such as total shifts, weekends worked, call burden, and overtime by physician. Even simple reviews will reveal patterns that would otherwise go unnoticed.
Leave inefficient scheduling in the past
Make your pagers history by choosing an automated scheduling solution tailored to your specialty.
Petal Automated Scheduling is proven to save time by simplifying schedules. Build and publish optimized schedules in minutes while reducing manual errors and administrative overhead. Proof: CHUM achieved 92% staff satisfaction using Petal Scheduling.
Here are three ways you’ll gain:
- Visualizing coverage gaps instantly with available, qualified providers and staff.
- Applying your unique department specific rules alongside personal preferences and absences.
- Identifying on-call staff quickly with the real-time calendar consolidated across departments or hospitals.
Smoother operations are within reach. Let’s transform your operation.
Have confidence in your security infrastructure:


