
Points clés à retenir
- Group billing doesn’t eliminate income control: Physicians retain influence over their earnings through compensation models tied to productivity and responsibilities.
- Modern compensation models promote fairness over equality: Hybrid structures balance individual performance with shared responsibilities, so high performers are rewarded.
- Technology enables successful group billing: Advanced tools like automation and real-time reporting simplify workflows, reduce errors, and help physicians track how their work becomes income.
Group medical billing does not reduce physician income, autonomy, or fairness. But beliefs to the contrary persist.
Modern group billing models are designed to improve billing transparency while rewarding performance and reducing administrative burden.
Yet, physicians hear rumours about peers’ group billing experiences—decreased autonomy, reduced revenue, and hampered decision-making among them. But facts matter! This is especially true when it comes to your finances.
Group billing can present major upsides, including valuable time saved for redirecting to more meaningful pursuits. Teams of clinicians share billing burden and reap the rewards collectively when they bill together. For many physicians, this is the ideal situation relative to their professional and personal goals.
Here are four group medical billing myths and what you should know before choosing between group and individual billing.
Do physicians lose control of their income with group billing?
Myth: Group billing created undue control over a physician’s income.
Reality: No, group billing doesn’t eliminate income control. Physicians influence earnings through structured compensation models tied to productivity and responsibilities.
Some folks think group billing is a black box: money goes in, but rewards don’t come out.
In fact, most group models are built around clearly defined internal distribution frameworks. These tie compensation to measurable inputs like clinical work and responsibilities, as well as strategic contributions. The key difference is that income is mediated through a structure rather than direct billing alone.
Billing distribution frameworks vary, but they’re rarely arbitrary. Your group may use productivity-based formulas, while others layer in factors like seniority or quality metrics. Transparency is critical to comfort in group billing: when physicians understand how revenue flows and how their activities relate to income, predictably replaces any sense of “lost control.”
Moreover, group billers prioritize “control” differently. Instead of managing every dollar tied to each encounter, physicians influence income through a broader set of levers: schedule design, patient mix, participation in group initiatives, and leadership roles. For many physicians, that expands financial opportunities.
There are three common group billing models in Canada:
- Salaried (shadow billing) model: Fixed salary independent of service volume. Billing is still submitted (shadow billed).
- Productivity-based splits: Income reflects individual billings or workload.
- Hybrid models: A base allocation plus performance-based adjustments is distributed.
Summary: Income control persists in a group scenario. Physicians participate in a structured system where income is shaped by established rules and shared risk.
Physicians using Petal gained $34,346 more annually on average compared to manual billing.
Do high-performing physicians subsidize others?
Myth: High-performing physicians are actually subsidizing others in a group billing environment.
Reality: No, high-performing physicians don’t subsidize others in most group billing models. Modern physician compensation structures tie a significant portion of income to individual productivity.
The myth suggests a flat pooling model where every group member gets the same share regardless of effort.
In fact, most modern group billing structures use hybrid compensation formulas designed to balance fairness with collaboration.
Hybrid models typically combine a productivity component with a shared pool. The productivity portion ensures that individual effort is directly recognized. The shared component supports group stability, covering collective responsibilities like teaching and coverage gaps. This dual structure aligns incentives without creating extreme income disparities. Hard workers see greater returns than slackers.
Here’s how hybrid compensation works in Canada:
- Individual component: Ties income to measurable productivity.
- Shared pool: Distributes value from collective responsibilities.
- Performance thresholds: Prevent sustained imbalance across members.
There’s a practical dimension to hybrid approaches: healthcare delivery often depends on interdependence. One physician’s efficiency may rely on another’s support. A purely individual model undervalues these contributions in a group scenario.
Notably, well-designed systems include safeguards. For example, minimum performance expectations ensure that persistent underperformance doesn’t go unchecked. The goal isn’t to punish but reflect the full scope of work required to run a successful practice.
Summary: High performers work within a model that rewards individual output while recognizing shared work that makes this output possible.
Is group billing more complicated than solo billing?
Myth: Group willing is plagued with complexity compared to solo billing due to multiple stakeholders involved.
Reality: Not for individual physicians. Group billing often simplifies admin burden by centralizing billing and compliance into dedicated systems or teams.
At first glance, group billing introduces additional layers to getting paid.
Shared accounts, internal tracking, and distribution processes feel more complex than individual billing. But with the right systems in place, much of the administrative burden is centralized.
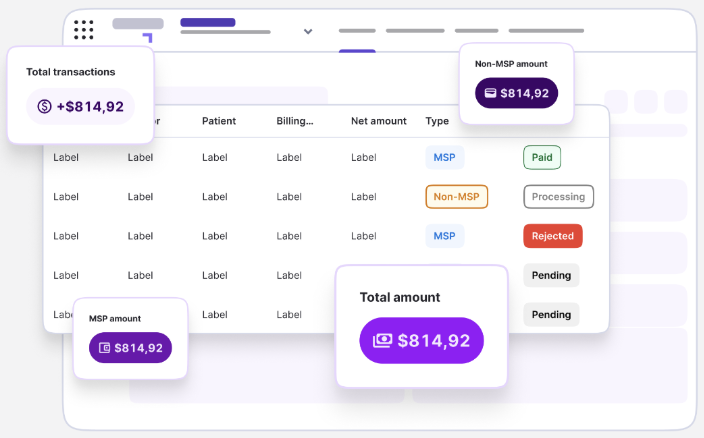
Billing, reconciliation, compliance, and reporting are managed through dedicated infrastructure. Physicians don’t manage these independently. In turn, duplication effort declines and accuracy improves as specialized teams (or tools) focus on these functions full-time.
- Remember: Medical billing is complicated no matter how you spin it. Whether individually or in a group, the most important thing to getting paid consistently and accurately is setting priorities and processes for first-pass acceptance.
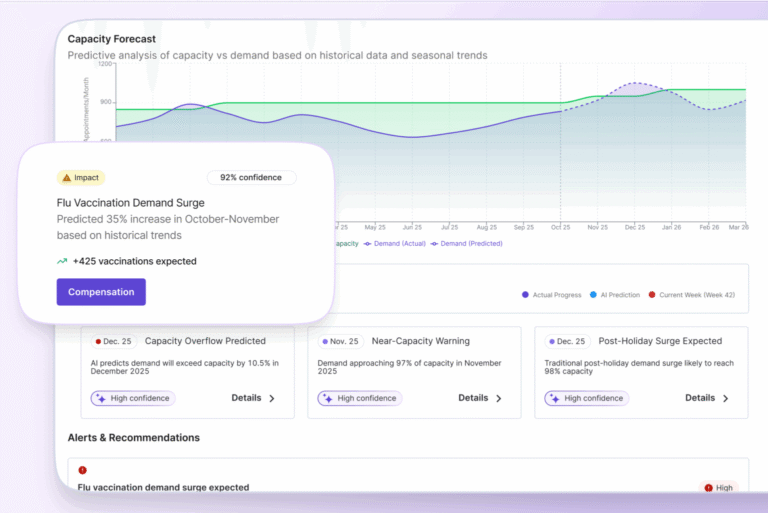
Technology is critical in easing group billing headaches. Modern practice management systems automate data capture, track productivity metrics, and generate transparent reports for each physician. Instead of juggling multiple administrative tasks, physicians interact with streamlined dashboards that show how their work translates into compensation.
At scale, complexity at the structural level becomes simple for individual group members.
Summary: Group billing shifts admin burden away from individual physicians and into systems designed to handle it efficiently.
12,000+ providers and clinics trust Petal to simplify their billing.
Does group billing reduce physician autonomy?
Myth: Group billing takes away the autonomous decision-making ability from physicians.
Reality: No, group billing doesn’t reduce autonomy. Most physician compensation models separate financial structure from day-to-day decision-making, allowing physicians to practice independently within a shared governance framework.
This myth conflates financial integration with professional independence.
In fact, group billing practices would have failed long ago if participants lost their autonomy—physicians are highly driven as individual professionals! In practice, well-structured groups separate governance from day-to-day clinical autonomy. Physicians retain control over how they practice.
To understand how autonomy persists, consider the governance structures of group billing. Many groups operate with elected committees. There are defined voting mechanisms and clear bylaws. These features outline how decisions are made concerning compensation changes, scheduling policies, and more. This creates a framework where physicians have a voice, rather than being subject to top-down control.
Here’s how this looks in practice:
- Clear decision pathways made known to all group members.
- Role clarity through collectively set organizational policies.
- Shared leverage where coordinated voices may carry more weight in negotiations.
Clinical autonomy typically remains intact.
Physicians continue to make decisions about independent decisions in the best interest of their patients and teams. Their clinic’s success remains in their hands.
Truth: Autonomy is reframed within a group billing system where individual clinicians cooperate through formal, shared governance structures.
Bring your medical billing into the 21st century
Still on the fence? We’ve got you covered either way.
Facturation médicale automates billing processes using tools designed for each province’s unique billing rules. If you or your group members need support, live agents are here.
- Impact in action: Physicians using Petal Billing reported an average revenue increase of 9.4% compared to manual billing. This equates to 161 hours saved annually at a value of $24,123 per year.
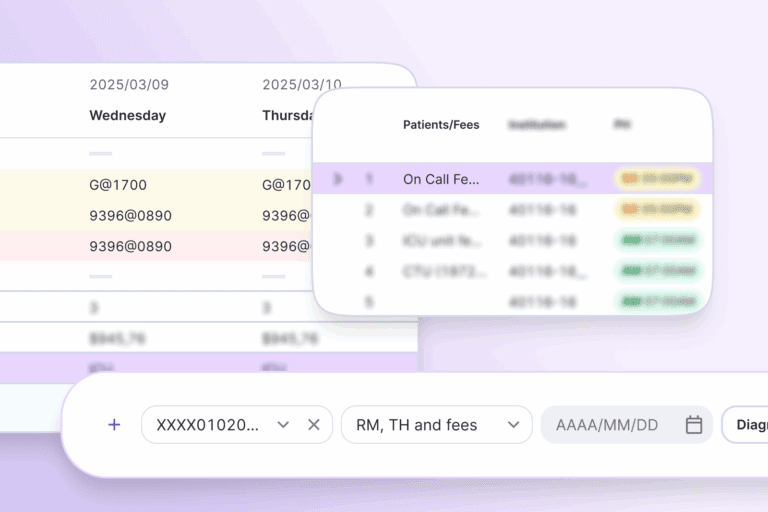
You’ll access stable, predictable revenue through end-to-end claim management guiding fewer billing rejections. Advanced features simplify billing, including provincial code validation, centralized billing for specialty groups, real-time claim status and remittance tracking, and more.
Whether solo or in a group, you deserve a solution tailored to your billing needs.
Improve your claim acceptance rate:
FAQ: Group medical billing
- What is group medical billing?
Group medical billing is a system where multiple physicians submit claims collectively and distribute revenue using a shared compensation model. - Is group billing more profitable than solo billing?
It depends on the model. Many physicians benefit from reduced admin time and improved claim accuracy, which in turn, increases income. - How do physicians get paid in group billing?
Compensation is typically based on a mix of individual productivity and shared responsibilities. This blend is often achieved through hybrid models. - Is group billing common in Canada?
Yes, especially in hospital-based specialties and large clinics where collaboration and shared infrastructure improve efficiency. - Does group billing affect clinical decision-making?
No. Physicians generally retain full clinical autonomy while they participate in shared financial structures.