
Points clés à retenir
- Policy and payment are out of sync: Canada promotes value-based care, but fee-for-service still dominates as providers’ preferred payment model.
- Progress is steady but slow: While FFS reliance declined from ~84% to ~70% over two decades, a system-wide tipping point still awaits.
- Physicians face conflicting incentives: Providers are expected to deliver coordinated and outcome-driven care while being paid for throughput and activity.
Canada’s healthcare system isn’t stuck.
But it is conflicted.
On paper, the direction is clear: value-based healthcare (VBC). Across provinces, policies increasingly emphasize outcomes, coordination, and sustainability. And rightly so as it focuses on maximizing patient outcomes relative to the cost of care, rather than the volume of services delivered.
This makes VBC the most sustainable model from a long-term perspective. It’s dedicated to proactive vs. reactive care that makes patient outcomes the priority.
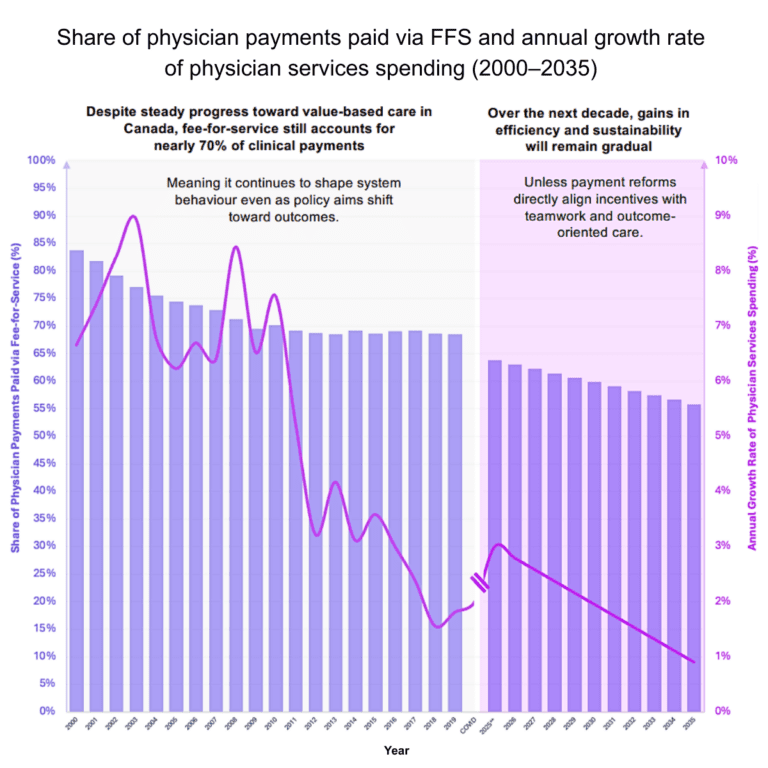
But one number tells a different story: Nearly 70% of physician payments are still tied to fee-for-service.
That’s the defining constraint on how fast the system can change. FFS has its merits, but relative to VBC goals, the popularity of FFS holds back Canada’s healthcare potential.
For health systems, payment is more than funding: it sets the limits for where and how care is provided.
What’s changing (and what isn’t)
Shifting away from FFS has taken more than 20 years to get to where we are now.
Canada reduced its reliance on FFS from roughly 84% of clinical payments in the early 2000s to around 69% today. That shift reflects years of experimentation with capitation, blended models, and alternative funding arrangements.
At the same time, something else happened:
- Growth in physician services spending—government spending on physicians compared to overall healthcare spending—slowed from 7% annually to 2%.
- Team-based care models expanded.
- Scope of practice conversations grew.
These aren’t coincidences. They’re signals. Payment reform is happening, but too slow to flip the system.
Because while the trend line is moving, the dominant signal to physicians hasn’t changed: Activity is still what gets paid.
The physician reality: Practicing between two systems
For physicians, this creates a daily contradiction.
On one hand, expectations are evolving. This includes the need to coordinate across care teams and specialists, dedicate more time to focused preventive care, manage complex, longitudinal care, and improve outcomes.
On the other hand, the financial model still rewards the volume of patient visits, number of procedures, and frequency of billable interactions.
That gap isn’t theoretical. It’s seen in how care is ultimately delivered.
Physicians are being asked to operate in a value-based system, while being paid to behave in a volume-based one. And when time, workload, and compensation are all under pressure, the system defaults to what it funds, which is understandable but not where VBC is found.
The administrative reality: Designing around misaligned incentives
The administrative reality lies in designing systems around fundamentally misaligned incentives. For healthcare administrators, the challenge is not simply operational; it’s structural.
Many of today’s transformation efforts are well-intentioned and strategically sound. Organizations are building interdisciplinary teams, expanding access points, integrating care pathways, and investing in digital tools to improve coordination.
However, they’re being implemented on top of a funding model that was never designed to support them. As a result, friction emerges across the system. Team-based models rely heavily on non-billable activities. Care coordination, while essential, often does not generate direct financial return. Preventive care reduces future demand yet doesn’t translate into immediate financial sustainability.
Compounding this challenge, governance and policy leaders often lack visibility into existing tools, such as the Petal Patient Hub, that can operationalize these intentions at scale, supporting both objectives and incentives, and turning strategic ambition into measurable system impact.
This leaves healthcare leaders in a difficult position, attempting to engineer VBC within a system still governed by volume-based economics. While success is possible, it tends to occur in isolated pockets, and scaling these efforts remains slow and complex.
Why this trend matters
At first glance, the decline of FFS appears to signal steady progress. And in many ways, it does. The share of payments tied to volume has been falling for years, alongside a slowdown in spending growth.
But that’s not the real story.
The system has not crossed a tipping point. FFS still accounts for roughly 70% of clinical payments, meaning it continues to shape behaviour, even as policy rhetoric shifts toward outcomes.
And until that tipping point is reached, transformation will remain incremental by design.
This matters because the system is entering a far more demanding phase. Workforce shortages are intensifying. Patient needs are becoming more complex. Fiscal constraints are tightening. And expectations for care demand and access continue to rise.
In that environment, efficiency is a requirement for sustainability.
But healthcare efficiency is often misunderstood. It does not come from doing more activity. It comes from organizing healthcare differently: coordinating across providers, intervening earlier, and ensuring patients see the right clinician at the right time.
We’ve seen the level of financial and patient impact that better patient navigation has provided through the Petal Patient Hub to the tune of hundreds of millions of dollars generated and hundreds of thousands of patients redirected away from emergency departments and to primary care.
In other words, it comes from VBC. And without the incentive structure to support it, those gains will remain limited.
What alternative payment models unlock
When payment models begin to shift, they do more than change how physicians are paid. They create operational freedom.
Freedom for physicians to spend time where it matters most, particularly with complex patients who don’t fit into short, billable encounters. Freedom for teams to coordinate care without the constant trade-off between collaboration and compensation. Freedom for non-physician providers to practice at the top of their scope of practice, expanding system capacity without expanding cost at the same rate.
At a system level, this shift also creates room to reallocate resources away from pure service volume and toward prevention, continuity, and long-term outcomes. This will in turn create a compounding effect of lower volumes for acute care and other specialist services down the road.
And the effects are real. Evidence consistently shows higher patient satisfaction, greater uptake of preventive services, and slower spending growth in team-based, value-oriented models.
This is why payment reform is the mechanism that determines whether transformation is possible at scale.
Clinicians save 3.1 hours per week using Petal Billing.
The critical insight: This will be a slow burn—unless something shifts
The question is no longer whether Canada will move toward VBC. That direction is already established in both policy and intent.
The real question is how long the system will tolerate the gap between what it says it wants and what it actually pays for.
Right now, the trajectory is clear. FFS is declining but gradually. Alternative models are expanding but unevenly. Innovation is happening. The challenge is that it is happening at the local level and not system-wide.
The result is predictable: progress without acceleration. And a gradual approach continues to put stress on patient outcomes and the system as a whole.
As long as FFS remains the dominant model, physicians will continue to navigate competing incentives between volume and value. Administrators will continue to design around constraints instead of through them. And system transformation will continue to lag system pressure.
The risk is not stagnation. It is falling behind the pace of need.
What this means for leaders right now
For physicians, this is no longer an abstract policy discussion; it’s a practical reality shaping day-to-day practice.
The question is how to deliver better care within a system that only partially supports it.
Increasingly, the answer lies in hybrid approaches: engaging in alternative payment models where available, embedding within team-based environments, and shifting toward longitudinal management of patient populations rather than episodic care.
For administrators, the challenge is more strategic and more urgent.
Where can incentives be aligned locally, even if they are not yet aligned system-wide?
That means rethinking compensation structures to support team-based care, investing in models that reduce reliance on pure volume, and identifying where flexibility already exists within current funding frameworks—and using it deliberately.
Because waiting for full system reform is not a strategy. It is a delay.
Recommendations to make an impact
Canada’s healthcare system is not resisting value-based healthcare. It is advancing toward it at exactly the speed its incentives allow. And today, those incentives remain largely anchored in fee-for-service.
Here are three recommendations to keep this momentum moving forward.
- Align incentives with intended outcomes:
- Invest in enabling infrastructure (supporting the adoption of operational tools at scale that make care coordination, patient navigation, and team-based care actionable
- Accelerate learning from what already works, replicating/inspiring from proven models.
That is the story behind the trend. Not whether value-based care works. Not whether there is policy alignment.
But whether the system is prepared to fund the behaviours it is asking for.
Until that answer changes, progress will continue. Just not fast enough.
Drive system-wide change through smarter, faster operations: