
Points clés à retenir
- Manual physician scheduling may feel familiar, but it often creates hidden operational costs, including administrative burden, unfilled appointments, provider frustration, and limited visibility across teams.
- Modernizing scheduling isn’t only a technology project. It requires process mapping, rule standardization, stakeholder alignment, and thoughtful change management.
- Hospitals and clinics reduce scheduling complexity by moving from disconnected spreadsheets and handwritten notes to a centralized, rules-based scheduling system.
Manual physician scheduling for hospitals, clinics, and medical groups continues to persist in a familiar mix of Excel files, handwritten notes, emails, phone calls, and last-minute text messages. The most effective way to modernize physician scheduling is to map your current process, identify scheduling bottlenecks, standardize scheduling rules, and transition to a centralized scheduling system.
It feels like the past 20 years of software and technology development has missed healthcare in lieu of spreadsheets and phone calls.
At first, this may seem manageable. Spreadsheets, as a tool, are ubiquitous. A coordinator knows the physicians. A clinic manager understands who is available, who prefers certain days, and which providers can cover specific appointment types.
At scale, even only a moderate increase, this system shows its weaknesses. As teams grow, locations expand, and patient demand changes, manual scheduling becomes harder to sustain.
One version of the schedule lives in Excel. Another is emailed to physicians. Time-off requests are tracked separately. Last-minute changes happen by phone or text. Appointment availability may not reflect real provider capacity.
The result is more than administrative inconvenience. Challenges to scheduling filling, underused clinical capacity, coverage gaps, provider frustration, and unnecessary time spent reconciling schedule changes, all start to pop up.
Here are four practical steps to help hospitals and clinics move away from manual physician scheduling and build a stronger foundation for operational efficiency.
1) Map the current physician scheduling process
Before changing the scheduling process, organizations need to understand how scheduling actually happens today.
In many clinical environments, the official process and the real process aren’t the same. The official process may say that schedules are created monthly in Excel and shared with providers. The real process may include additional emails, informal physician preferences, handwritten notes, separate vacation calendars, phone calls to confirm availability, and manual updates after every change.
This is why the first step is to map the full scheduling workflow from start to finish.
Start by identifying:
- Who creates the schedule
- Where physician availability is collected
- How vacation and time-off requests are submitted
- How call rotations, clinic shifts, and appointment coverage are assigned
- How changes are communicated
- Where the final schedule is stored
- Who has access to the most recent version
- How appointment availability is connected to provider schedules
The aim of this exercise is to reveal how much work happens outside the spreadsheet.
For example, a scheduling coordinator may spend hours checking whether a physician is available before confirming clinic coverage. A department manager may manually compare schedules across locations. A provider may rely on an outdated version of the schedule because the latest change was sent in a separate email thread.
These gaps matter because they create delays, duplicate work, and cause uncertainty.
The goal isn’t to criticize the current process. In many cases, manual scheduling exists because teams have done their best with the tools available. The goal is to identify where the process is no longer supporting the complexity of modern healthcare operations.
25,000+ physicians leverage Petal Workforce to reduce scheduling burden.
2) Identify the highest-friction scheduling problems
The truth is you can’t tackle everything at once. But you can start with the actions that have the largest upfront impact.
Once the current process is mapped, the next step is to identify the scheduling problems that create the greatest operational benefit.
Remember: Not every scheduling issue has the same weight. Some are minor inconveniences. Others directly affect appointment access, provider workload, administrative efficiency, and patient flow.
Common signs of high-friction scheduling include:
- Schedules take too long to build or update
- Appointment slots remain unfilled despite provider availability
- Physicians receive conflicting or outdated schedule information
- Coverage gaps are discovered too late
- Time-off requests are difficult to reconcile
For hospitals and clinics, these issues have a direct effect on performance.
If a provider’s availability isn’t clearly visible, appointment slots have a tendency to go unused. If schedule changes aren’t updated in real time, patients may be booked into the wrong availability. If physicians don’t trust the schedule, they may spend more time checking, questioning, correcting, or, worst of all, not using it at all.
Manual scheduling also makes it harder to manage fairness and workload distribution. Without clear rules and visibility, some providers may feel they are receiving less desirable shifts, more call responsibilities, or inconsistent scheduling treatment.
This is where change management becomes important.
For example, the priority may be to reduce schedule creation time. Or it may be to improve appointment fill rates. Or it may be to reduce last-minute coverage issues across multiple locations.
Clear priorities help teams avoid a common mistake: trying to fix everything at once.
Instead, focus on the problems that create the greatest burden and the clearest business case for change.
3) Standardize scheduling rules before automating
Automation works best when the rules are clear.
If a clinic moves from Excel to a scheduling platform without first defining its scheduling rules, the same confusion may continue in a new system. The technology may be better, but the underlying process remains unclear.
That is why standardization is a critical step before automation.
Physician scheduling rules may include:
- Minimum and maximum shift requirements
- Clinic coverage needs by location
- Call rotation requirements
- Rules for evenings, weekends, or holidays
- Vacation and time-off approval processes
- Union or collective bargaining agreement standards
- Specialty-specific coverage requirements
Standardizing these rules reduces ambiguity. It also makes the scheduling process easier to explain, manage, and improve.
This step is especially important for physician buy-in.
When schedules are managed manually, many rules may live in someone’s head—but when those rules aren’t documented, the process becomes difficult to scale and easy to question.
By documenting scheduling rules, organizations create a more transparent system. Physicians better understand how schedules are built. Managers make more consistent decisions. Administrative teams reduce the back-and-forth required to resolve conflicts.
Standardization also supports better change management. Teams are more likely to adopt a new scheduling process when they understand the logic behind it.
Before introducing a new system, bring key stakeholders into the conversation.
Ask practical questions:
- Which rules are essential?
- Which rules are preferences rather than requirements?
- Where do exceptions happen most often?
- Which scheduling decisions create the most conflict?
- What information does each stakeholder need to trust the schedule?
The answers will help create a scheduling model that is both operationally sound and easier to adopt.
CHUM saves 8,000+ hours per year using Petal Workforce.
4) Move to a centralized, automated scheduling system
After mapping the process, identifying pain points, and standardizing rules, organizations are better prepared to move from manual scheduling to a centralized system.
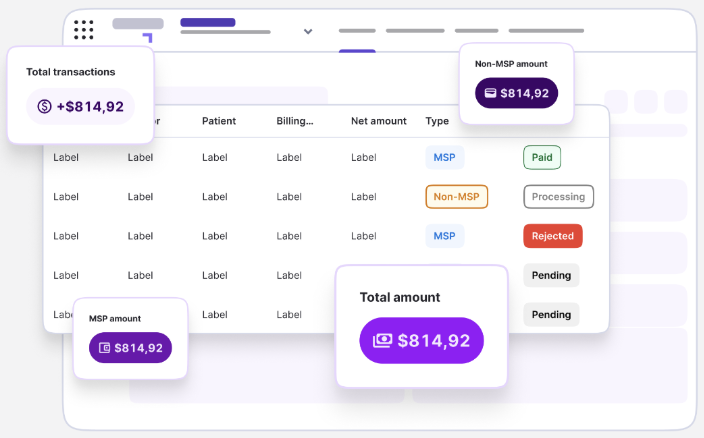
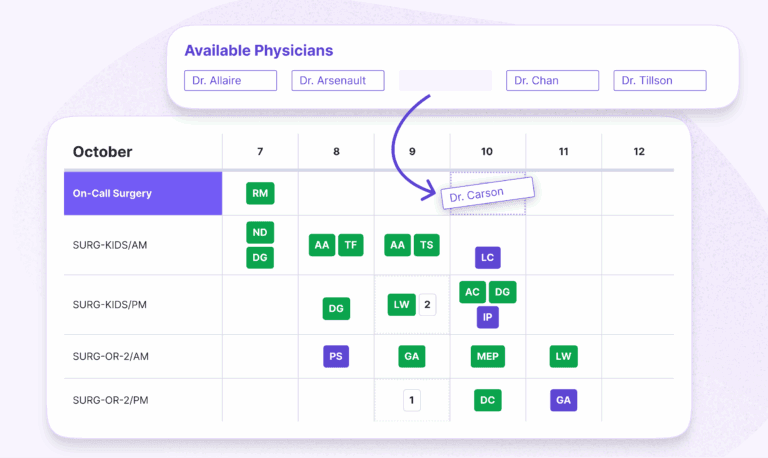
The goal is to create one reliable source of truth for physician schedules.
A modern scheduling system should help teams manage provider availability, schedule rules, time-off requests, shift assignments, and changes in a more connected way. Instead of relying on multiple spreadsheets and email threads, stakeholders can access the most up-to-date schedule from one place.
This supports several operational improvements.
First, it reduces administrative burden. Scheduling teams spend less time manually updating files, reconciling conflicting versions, and communicating every change individually.
Second, it improves visibility. Managers better understand provider availability, clinic coverage, and schedule gaps before they affect operations.
Third, it helps improve appointment access. When physician availability is clearer and easier to manage, organizations can better align provider capacity with patient demand.
Fourth, it supports provider engagement. Physicians have greater confidence that schedules are accurate, rules are applied consistently, and changes are easier to request or track.
However, implementation should be gradual and intentional.
A successful transition may begin with one department, one specialty, or one scheduling workflow. This allows the organization to test rules, gather feedback, adjust processes, and demonstrate value before expanding.
Common mistakes to avoid when modernizing physician scheduling
Many organizations recognize that manual scheduling is no longer sustainable, but their transition still stalls if the change isn’t managed carefully.
One common mistake is automating too quickly without first cleaning up the process. If scheduling rules are unclear, automation may reproduce the same problems faster.
Another mistake is excluding physicians from the design process. Physician schedules directly affect workload, work-life balance, and clinic flow. Their input is essential for adoption.
A third mistake is under estimating communication. Teams need to know what is changing, when it is changing, and how the new process will affect their day-to-day work.
Finally, some organizations focus only on schedule creation and overlook ongoing schedule management. In healthcare, schedules aren’t static. Time-off requests, coverage changes, patient demand, and provider availability shift frequently.
Making the automated and transparent change
Manual physician scheduling may have worked when teams were smaller, schedules were simpler, and changes were easier to manage.
But for today’s healthcare organizations, spreadsheets and handwritten processes create more complexity than control.
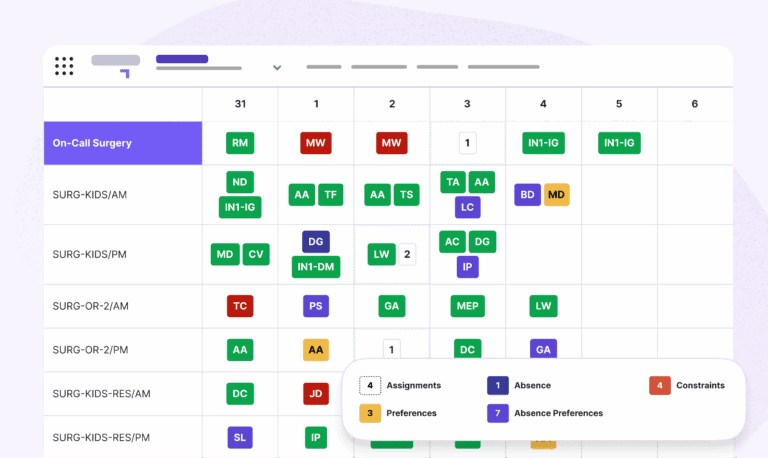
That’s why Petal Automated Scheduling simplifies the layered rules, preferences, and constraints that make healthcare scheduling difficult.
Modernizing physician scheduling requires more than replacing Excel. Petal allows teams to perform a structured approach:
- Mapping the current process
- Identifying the highest-friction problems
- Standardizing scheduling rules
- Moving to a centralized system that supports visibility
With the right process and the right technology, physician scheduling is less reactive, more transparent, and better aligned with patient access and clinical capacity.
Contact a Petal scheduling expert to save your team time and frustration today.
Discover the difference that personalization makes:
FAQs: Replacing manual scheduling
Why is manual physician scheduling a problem?
Manual physician scheduling often depends on spreadsheets, emails, phone calls, and individual knowledge. This can lead to outdated schedules, duplicate work, coverage gaps, appointment availability issues, and frustration for physicians and administrative teams.
How can clinics move away from Excel-based physician scheduling?
Clinics can start by mapping the current scheduling process, identifying the biggest sources of friction, documenting scheduling rules, and gradually moving to a centralized scheduling system that provides real-time visibility and automation.
What should be standardized before automating physician schedules?
Organizations should standardize rules for physician availability, time off, call rotations, clinic coverage, shift distribution, appointment types, provider preferences, and approval workflows before introducing automation.
How does automated physician scheduling improve clinic operations?
Automated scheduling can reduce manual work, improve schedule visibility, support better appointment capacity planning, reduce last-minute conflicts, and help teams manage provider availability more efficiently.
Is physician scheduling modernization only a software project?
No. Scheduling modernization is both a process improvement and a change-management initiative. Technology is important, but success also depends on stakeholder alignment, clear rules, communication, and adoption by physicians and staff.