


Points clés à retenir
- Legacy tools persist despite better alternatives: Fax machines and pagers remain embedded due to interoperability gaps, regulatory familiarity, and workflow inertia—not because they’re efficient.
- Administrative friction is the bigger hidden cost: Manual scheduling and paper-based intake systems quietly consume hours, introduce errors, and delay care across the patient journey.
- Modernization delivers immediate operational gains: Replacing outdated tools improves coordination and seamlessly unlocks time across care teams.
Fax machines still exist in healthcare because they solve interoperability gaps, are widely accepted for compliance, and are deeply embedded in clinical workflows.
But they persist at the cost of efficiency. As communication slows and administrative burden increases, care becomes delayed.
Things change. It’s inevitable, especially in healthcare. Processes change, people move on, and technology becomes obsolete. Obsolete not because the use case no longer exists, but because a better solution was developed. At the turn of the 20th Century, we still had to get from point A to point B, but we were quickly speeding into the age of the automobile instead of a horse and buggy.
Now, physicians in Canada are losing nearly 20 million hours annually to admin burden. And with 53% of physicians saying admin workload has increased in the past 12 months, we need to reduce the trend before even more physicians become burnt-out.
The reality is that countless healthcare organizations still rely on tools that haven’t meaningfully evolved in decades, even if better tools and systems have been created to do it better.
Fax machines. Pagers. Paper forms. Manual scheduling logs.
These systems persist not because they’re efficient, but because they’re deeply embedded. They sit at the intersection of compliance, habit, and fragmented infrastructure, making them difficult to replace, even when better options exist that save time, money, and expand access to care.
Understanding why they’ve lasted this long is the first step to replacing them.
1) Why do fax machines still exist in healthcare?
Fax machines still exist because they act as a universal communication method across disconnected healthcare systems. They’re considered compliant and are embedded in long-standing workflows.
Fax machines are one of the most visible symbols of healthcare’s attachment to legacy tools, and for good reason. In an era of cloud computing, it’s not unusual for patient referrals, lab results, and discharge summaries to still be sent via fax. The fax machine was invented in 1964. We’re still using a solution that debuted when only 3% of households had a colour television. Why?
Why fax persists:
- Interoperability gaps: Healthcare systems often don’t communicate seamlessly. Fax acts as a lowest-common-denominator channel that “works with everything.”
- Regulatory familiarity: Fax is widely accepted as compliant with privacy regulations when used correctly, reducing perceived legal risk.
- Workflow inertia: Clinics, hospitals, and administrative teams have built processes around fax over decades. Replacing it requires coordination across multiple stakeholders.
The hidden cost:
Fax may be universal, but it’s far from efficient. Staff must manually send, receive, sort, scan, and re-enter information. Errors are common: missing pages, illegible text, or misdirected transmissions.
This creates downstream impacts:
- Delayed referrals and care coordination
- Increased administrative workload
- Higher risk of lost or incomplete information
What replaces faxing:
Digital referral networks, secure document exchange platforms, and integrated EHR workflows eliminate many of these friction points. The challenge? Aligning stakeholders to adopt it simultaneously.
CHUM saves 8,000+ hours per year using Petal Workforce.
2) Pagers: Reliability over functionality
Pagers feel even more anachronistic than fax machines. Even with a device 5,000 times more powerful than the top super computers of 1985 in every physicians’ pocket in a smartphone, pagers remain common in hospitals and acute care settings.
Why pagers still exist:
- Signal reliability: Pager networks often function in areas where cellular networks struggle, including basements and thick-walled hospital buildings.
- Simplicity: They deliver one core function—alerts—without distractions or complexity.
- Redundancy: In critical environments, having a backup communication system is seen as essential.
The trade-off:
While reliable, pagers are fundamentally one-way communication tools. They lack context, require follow-up calls, and create delays in urgent situations. Overall, their limited functionality doesn’t meet today’s complex needs.
This leads to:
- Communication bottlenecks
- Inefficient care coordination
- Interrupt-driven workflows that increase cognitive load
Where the shift is happening:
Secure clinical messaging platforms are increasingly replacing pagers by combining reliability with richer functionality through on-call and callout solutions that create read receipts, patient context, and team-based communication.
The transition is gradual, but the direction is clear: systems that enable real-time, two-way communication reduce friction across care teams.
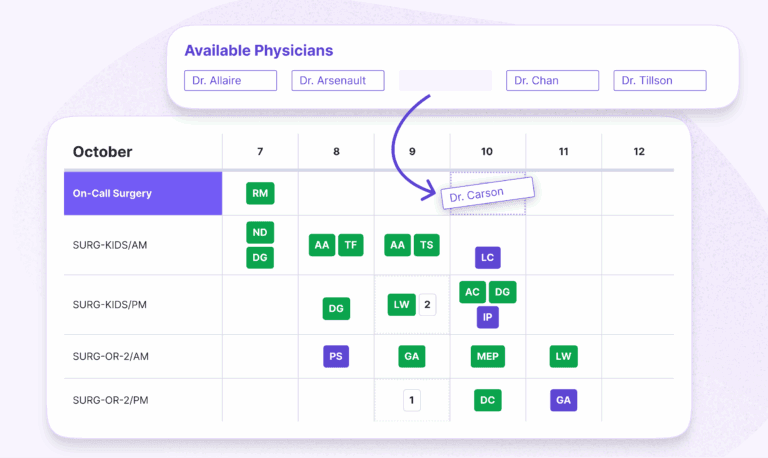
CHUM reduced scheduling time by 98% using Petal.
3) Manual scheduling systems: The invisible time drain
Not all outdated tools are as obvious as fax machines or pagers. Some of the most persistent inefficiencies live in administrative workflows, especially scheduling.
In many organizations, scheduling still relies on spreadsheets, whiteboards, disconnected systems, and the always ubiquitous Post-It Note.
Why it persists:
- Customization needs: Scheduling is complex and highly specific to each department or practice.
- Legacy processes: Staff are trained on existing systems and hesitant to switch.
- Perceived risk: Errors in scheduling directly impact operations, making teams cautious about change.
The impact:
Manual scheduling creates inefficiencies that compound over time:
- Hours spent coordinating shifts, on-call rotations, and coverage
- Increased risk of errors and double-bookings
- Limited visibility into staffing gaps or overload
These inefficiencies ripple beyond the administrator, scheduler, nurse, or physician and into patient care through delays, understaffing, or burnout.
The modern alternative:
Automated scheduling platforms centralize availability, enforce rules, and optimize coverage in real time. What once took hours can often be reduced to minutes with better accuracy and transparency.
4) Paper-based intake and forms: Friction at the front door
Patient intake is another area where outdated tools quietly persist. Paper forms, clipboards, and manual data entry remain common across clinics and hospitals.
Why it hasn’t changed:
- Accessibility assumptions: Paper is seen as universally accessible for patients of all demographics.
- Integration challenges: Digital intake systems must connect with existing EHRs and workflows.
- Change management: Front-desk processes are deeply ingrained and difficult to redesign.
The downstream effects:
Paper-based intake introduces friction at the very start of the patient journey:
- Longer wait times and administrative bottlenecks
- Data entry errors and duplication
- Delayed access to patient information for clinicians
This is one of the few areas where inefficiency is immediately visible to patients—shaping their perception of the entire care experience.
What replaces it:
Digital intake solutions allow patients to complete forms in advance, reduce redundancy, and ensure data flows directly into clinical systems. The result is faster throughput and cleaner data from the outset.
Why these tools persist and why that’s changing
Across all four examples, a common pattern emerges:
- They work “well enough” to avoid urgent replacement.
- They’re embedded in complex systems that are difficult to untangle.
- They carry low perceived risk compared to introducing new workflows.
But that equation is shifting. Modernization demands performance.
Healthcare organizations are facing increasing pressure—from workforce shortages to rising administrative costs—to operate more efficiently. Small inefficiencies that were once tolerable are now material.
When multiplied across hundreds of staff and thousands of interactions, outdated tools translate into:
- Lost time
- Delayed care
- Reduced capacity
Where to start: replacing friction, not everything at once
The goal isn’t to overhaul every system overnight. The most effective approach is targeted: identify where friction is highest and where improvements will have immediate impact.
A practical starting point:
- Map your workflows: Identify where manual steps, delays, or duplication occur
- Quantify the time spent: Even small inefficiencies add up quickly
- Prioritize high-impact areas: Communication, scheduling, and intake often deliver the fastest returns
In many cases, administrative workflows offer the clearest path to ROI. They’re easier to modernize than clinical systems and deliver measurable improvements in both time and coordination.
Moving forward: From legacy tools to connected systems
Fax machines and pagers haven’t survived because they’re effective—they’ve survived because they’re embedded.
But as healthcare becomes more connected, their limitations are harder to ignore.
The shift isn’t just about replacing old tools with new ones. It’s about moving from fragmented, manual processes to integrated systems that support how care is actually delivered today.
Organizations that make that transition gain more than efficiency. They unlock capacity that frees up time, reduces friction, and enables teams to focus on higher-value work.
And in today’s healthcare environment, that’s not just an operational advantage. It’s a necessity.
Ready to say good-bye to pagers? Contact a Petal scheduling expert to launch your digital transformation.
FAQ: Fax machines in healthcare
- Why are fax machines still used in healthcare?
Fax persists due to interoperability gaps, regulatory familiarity, and entrenched workflows. - Are fax machines HIPAA compliant?
Yes, when used correctly, fax is considered compliant, which contributes to its continued use. - What is replacing fax in healthcare?
Digital referral networks, secure document exchange platforms, and EHR-integrated workflows. - Why are pagers still used in hospitals?
They are reliable in low-signal environments and serve as a backup communication system. - What are the biggest inefficiencies in healthcare operations?
Manual scheduling, paper-based intake, and fragmented communication systems.


