


Points clés à retenir
- Burnout is driven by system friction: Canadian physicians spend nearly 10 hours per week per physician on admin with much of it tied to scheduling and coordination.
- Scheduling is a major and fixable driver of burnout: 56% of physicians report scheduling challenges as a barrier to their health and wellness.
- Better scheduling unlocks time, revenue, and capacity: When scheduling aligns with documentation and billing, physicians save even more time for redirecting to other programs and pursuits.
Physician burnout is usually caused by operational friction. Poor physician scheduling creates downstream issues from documentation delays to uneven coverage and administrative overload. The most effective physician groups reduce burnout by improving schedules at source.
For most physicians, scheduling is supposed to be a problem of logistics. It’s now become a clinical one.
When schedules break down, especially when coverage is uneven, clinics are overbooked, or changes happen last minute. This creates downstream effects that are felt quickly. Documentation gets rushed. Billing details get missed. Follow-ups fall through. This is where burnout quietly takes hold.
Across Canada, physicians now spend close to 20 million hours annually on administrative work. In fact, that burden often amounts to roughly 10 hours per week per physician.
Given that 46% of Canada’s physicians report high levels of burnout and 49% of family doctors work beyond capacity, unlocking clinical time is critical to stopping the steady erosion of physician well-being.
The solution is redesigning how scheduling and processes work within your practice or group. Below is a practical, physician-centered framework to do exactly that.
Step 1: Start by reframing scheduling as a system
Most scheduling problems are treated reactively. Someone calls in sick, a shift needs coverage, a clinic runs over capacity, and the fix is manual coordination. This means someone is tasked with extensive outreach that includes phone calls, texts, emails, spreadsheets, or last-minute compromises.
On a small scale, this feels manageable. At the group scale, it becomes unsustainable.
What high-functioning groups recognize early is that variability, not volume, is what breaks scheduling systems. The more clinicians, sites, and care environments involved, the more fragile manual coordination becomes.
This is why physician scheduling software should be treated as infrastructure instead of administration.
When it isn’t, the burden lands on physicians:
- You stay late to finish notes because the clinic ran over.
- You handle coordination gaps between teams.
- You compensate for uneven coverage.
Impact: Reframing replaces what many physicians describe as “invisible work,” where effort informally tracked accumulates daily. This is the first step to removing that burden.
Step 2: Build real visibility into capacity and demand
One of the biggest drivers of scheduling stress is simply not knowing what’s happening across the system.
When schedules live in silos, or are updated manually, coordination becomes reactive. Physicians and administrators spend time chasing availability, clarifying rules, and resolving conflicts that could have been prevented.
This is where operational visibility becomes critical.
Decision-making completely changes when teams have a real-time view of who’s available, where gaps exist, and how demand shifts day-to-day and week-to-week.
Instead of reacting to problems, you prevent them. For physicians, the benefit is simple: fewer surprises, fewer interruptions, and fewer after-hours fixes.
In practice, this means:
- Transparent schedules that update in real time.
- Shared visibility across clinics or departments.
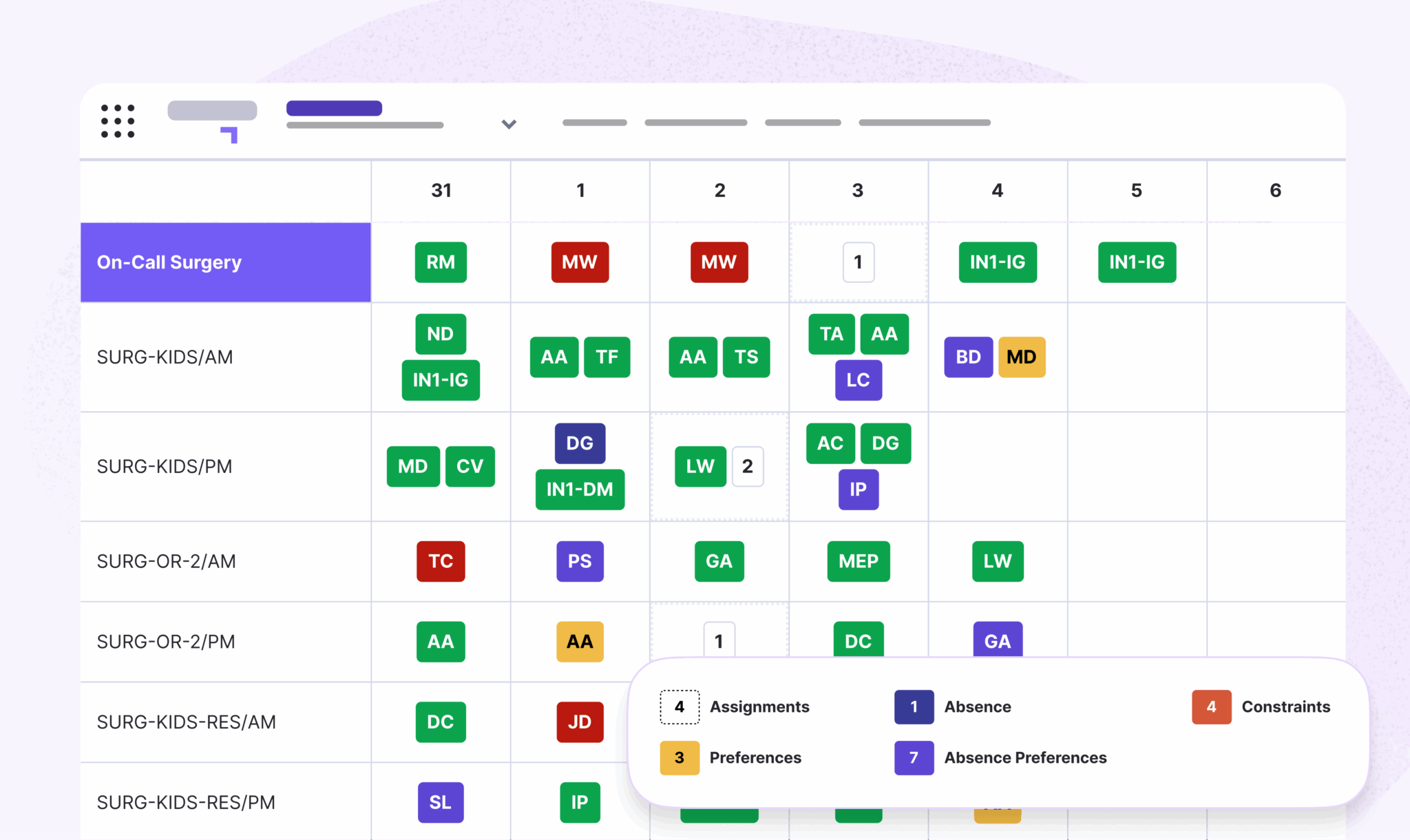
- Clear rules embedded into scheduling (i.e. union rules, specialties, coverage requirements, constraints).
Impact: Greater scheduling visibility reduces reactive coordination and gives physicians more predictability in their day-to-day workflows.
37,000+ physicians leverage Petal Workforce to reduce scheduling burden.
Step 3: Reduce cognitive load through automation
Burnout describes the mental fragmentation of jumping from one task to another. For clinicians, this includes extensive dedication to tasks outside of providing care.
You’re adding cognitive load every time you check multiple systems for availability or coordinate coverage manually. Resolving schedule conflicts causes mental fatigue. Documentation updates after a chaotic clinic session are unreasonably dreaded.
This “context switching” is one of the most underestimated contributors to physician fatigue. And importantly, much of this work is predictable. That’s what makes it ideal for automation in clinic operations.
High-performing groups redesign scheduling so that:
- Rules are embedded directly into the system.
- Conflicts are flagged automatically.
- Shift swaps happen within defined guardrails.
- Scheduling aligns with downstream workflows (like billing and documentation).
This reduces the need for constant decision making.
It’s also worth noting that over half of physicians (56%) report scheduling challenges as a barrier to maintaining their health and wellness. When automation reduces that friction, it moves from simply an operational improvement to a direct intervention on burnout.
Impact: Automation reduces the cognitive burden of constant schedule management. In turn, physicians spend less time coordinating logistics and more time focused on patient care.
Step 4: Align scheduling with documentation and billing
One of the most overlooked realities in clinical practice is how tightly scheduling affects everything downstream. Take a moment to imagine the cascading effects of scheduling on the operations of a clinic, department, and most importantly, on patient care. These effects include:
- Drops in documentation quality.
- Increases in billing errors.
- A slip in submission timelines.
- Less predictable revenue.
This is a scheduling problem. High-functioning physician groups treat scheduling, documentation, and billing as a single system.
That means structuring clinics in a way that allows time for proper documentation, balancing coverage to reduce rushed encounters, and ensuring scheduling supports consistent submission timelines.
Just as importantly, it involves looking upstream and using patterns like billing rejection rates to address the scheduling and workflow issues that created them in the first place. Better schedules don’t only protect time; they protect the entire operational flow of care.
Impact: When scheduling aligns with documentation and billing workflows, organizations reduce administrative rework toward improving revenue consistency and decreasing downstream inefficiencies.
Petal Workforce generates $610,000 in direct benefits per year at CHUM.
Step 5: Measure success in time reclaimed
Many operational improvements focus on productivity metrics: more patients seen, faster throughput, higher revenue. Those matter but they miss the physician experience.
A more meaningful metric is time reclaimed.
Time reclaimed looks like:
- Leaving on time more consistently.
- Spending less time on administrative follow-up.
- Having space to document properly during the day.
- Reducing after-hours work.
At scale, this becomes measurable.
For example, improved scheduling and workflow design saves hundreds of hours annually per group, returns meaningful time to physicians each week, and increases capacity without increasing workload.
For consideration: If physicians in Canada we able to free up only one-third of their administrative burden, it would create the equivalent capacity to adding 7,000 new physicians to the system. Not to mention the added benefit of more time needed rest and balance for clinicians.
This is where operational improvement and physician well-being finally align.
Impact: Measuring time reclaimed instead of pure output helps organizations build more sustainable physician workloads while improving retention and long-term clinical capacity.
Go from manual schedules to protected capacity
There is no single fix for physician burnout. The system is too complex for that.
But there is a pattern among physician groups that are getting this right.
They stop treating scheduling as an isolated administrative function—and start treating it as a core part of clinical capacity management.
Petal Automatisation des horaires is proven to save time by simplifying schedules. Build and publish optimized schedules in minutes while reducing manual errors and administrative overhead.
- Proof: CHUM used Petal Workforce to transform its operations. An independent study analyzed the impacts:
- 8,000 hours saved annually
- $610K in annual economic value
- 407% increase in daily self-service searches
Ultimately, your goal is protecting the one resource the system cannot afford to lose: physician time.
Explore how Petal scheduling experts can simplify your scheduling workflows to unlock more time for patients without burdening staff.
FAQ: Physician scheduling and burnout
How does physician scheduling contribute to burnout?
Poor scheduling increases administrative burden, creates documentation delays, causes uneven workloads, and forces physicians to spend more time coordinating care outside clinical hours.
What are the biggest scheduling challenges in healthcare?
Common challenges include last-minute coverage gaps, manual scheduling processes, inconsistent visibility across departments, and disconnected billing or documentation workflows.
Can scheduling software reduce physician burnout?
Yes. Scheduling software can reduce manual coordination, automate conflict resolution, improve visibility into staffing gaps, and reduce administrative workload for clinicians.
Why is scheduling visibility important in healthcare operations?
Real-time visibility helps healthcare organizations identify staffing gaps early, balance workloads more effectively, and avoid operational disruptions that increase clinician stress.
What metrics should healthcare organizations track for physician scheduling?
Important metrics include time reclaimed, after-hours administrative work, schedule creation time, physician satisfaction, clinic utilization, and billing efficiency.
How does scheduling affect healthcare revenue?
Poor scheduling can lead to documentation delays, billing errors, missed submissions, and uneven clinic utilization, all of which affect financial performance.


